CASE REPORT | https://doi.org/10.5005/jp-journals-10055-0060 |
An Unusual Presentation of Epidermoid Cyst: A Case Report
1–3Department of Surgery, Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, Punjab, India
Corresponding Author: Jotdeep S Bamrah, Department of Surgery, Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, Punjab, India, Phone: +91 8427700736, e-mail: jotdeepbamrah@yahoo.com
How to cite this article Bamrah JS, Ded KS, Bhargava GS, et al. An Unusual Presentation of Epidermoid Cyst: A Case Report. AMEI’s Curr Trends Diagn Treat 2019;3(1):35–36.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Penile cysts are uncommon. A case of a 5-year-old boy with an epidermoid cyst of the penis is reported. He was found to have an asymptomatic soft mass at the dorsum of his penis. Preoperative differential diagnosis of the epidermoid cyst and the dermoid cyst was considered. Excision of the mass was performed, and the diagnosis of epidermoid cyst in the penis was made that was confirmed on histopathological examination. In such cases, clinicians should manage patients either by observation or excision of the cyst.
Keywords: Dermoid cyst, Epidermoid cyst, Penile cyst.
INTRODUCTION
Epidermoid cysts are developmental cysts. They may arise due to entrapment of pluripotent cells or as a result of implantation of the epithelium. Cutaneous epidermoid cysts may arise from all parts of the body, but penile epidermoid cysts are very uncommon. Most are encountered in childhood1 and are usually congenital. However, the etiology of penile epidermoid cysts in the elderly is not well understood. In previously reported cases, a penile epidermoid cyst has been described as a slowly growing mass.1–3 It has been reported that the period of growth varies from 2 to 8 years.2,3 We present a case of a gradually growing penile epidermoid cyst that developed in a 5-year period of time.
CASE DESCRIPTION
A 5-year-old boy was found to have an asymptomatic, slowly growing soft mass measuring 2 × 1.5 × 1 cm in the dorsum of his penis on external examination (Fig. 1). He had no history of trauma, inflammation, urinary tract infection, hematuria, or dysuria. The elastic mass was globular in shape, soft, nontender, nonpulsatile, freely movable within the dermis, and had a smooth surface, with normal overlying skin.
Preoperative differential diagnosis of the epidermoid cyst and the dermoid cyst was considered. There was neither a keratin-filled punctum nor any signs of inflammation. Excision of the cyst was performed under general anesthesia through a linear incision (Figs 2 and 3).
A cystic mass of 4 × 2 × 1.5 cm size was excised (Fig. 4). Macroscopically, the cut surface of the mass appeared to be full of a cheesy material, and both cytology and culture results were negative. The incision was closed with absorbable suture (Fig. 5).
Histological examination revealed that the wall of the cyst was lined with stratified squamous epithelium and laminated keratin. It did not contain either skin appendages or germ cells. The final diagnosis was the epidermoid cyst of the penis.

Fig. 1: Penile swelling on external examination

Fig. 2: Cystic swelling protruding out from incision site
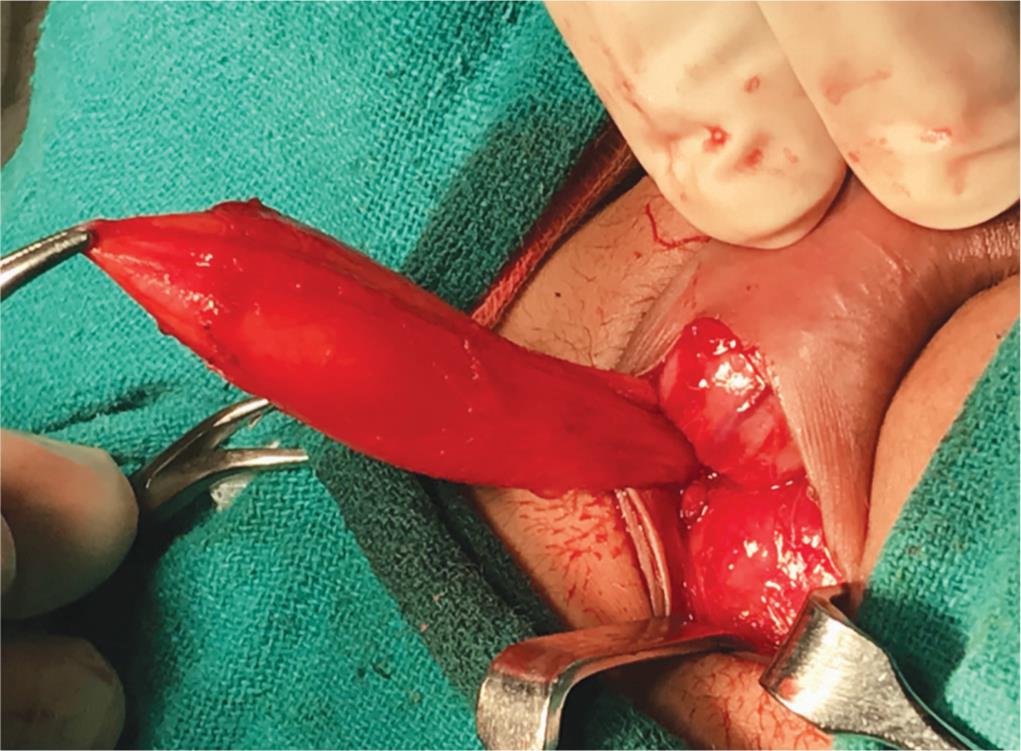
Fig. 3: Dissection showing depth of cyst up to pubic symphysis
DISCUSSION
Epidermal cysts are common benign tumors that may arise from the infundibular portion of the hair follicle spontaneously or subsequent to trauma, but penile epidermoid cysts are uncommon and usually congenital. The etiology is not clear. Some authors have adduced that it may develop from the median raphe cyst, following an abnormal closure of the median raphe during embryogenesis.3 Others have suggested that median raphe cysts are a different entity from epidermoid cysts.4 These cysts may occur because of occluded hair follicles, the mechanical implantation such as that involving injection of epidermal fragments, and obstructed eccrine ducts.2 The present case is more likely to have originated from a median raphe cyst because of the patient’s age and the development of the cyst over a long period of time. The penile epidermoid cyst can be diagnosed by a careful examination with evaluation by ultrasonography and/or computerized tomography or magnetic resonance imaging. Dermoid cyst, teratoma, and urethral diverticula should be considered in the differential diagnosis of the epidermoid cyst.2 An epidermal cyst is lined by the well-developed stratified epithelium, and often contains keratin, which can be expressed from the cyst, while a dermoid cyst contains skin and skin appendages, and a teratoma contains derivatives from other germ cells. Therefore, these lesions can be distinguished from an epidermoid cyst. Unlike the urethral diverticula, such cysts do not have a connection with the urethra.
Although epidermoid cysts are benign lesions, neoplastic transformation of their epithelium has been reported to occur rarely.5,6 No cases of malignancy arising in the wall of an epidermoid cyst of the penis have been reported previously.1,3 The best treatment of penile epidermoid cysts is total excision. Local recurrence has not been reported after complete excision of the cyst. There were no findings of malignancy in our case, similar to that reported by others.1,3 Although malignant transformation is very rare, it should be kept in mind and following excision of an epidermoid cyst, patients should undergo a long-term follow-up.
CONCLUSION
In conclusion, epidermoid cyst of the penis is rare; in the pediatric age group, it can occur congenitally after a seemingly minor surgical procedure such as circumcision. The swelling may remain largely asymptomatic unless secondarily infected. Care needs to be taken while performing even minor surgical procedures to avoid this complication. The condition should be treated by complete excision. The rare possibility of malignant transformation must be borne in mind.
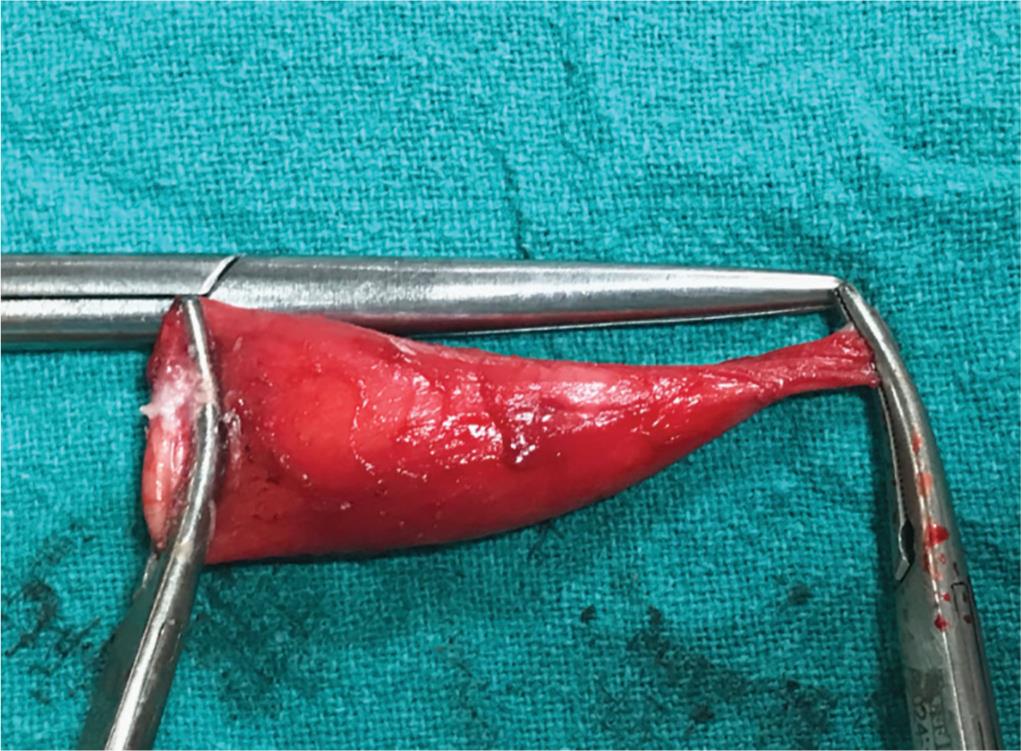
Fig. 4: Excised cyst of 4 x 2 x 1.5 cm size filled with cheesy material, confirmed to be epidermoid cyst on HPE

Fig. 5: Closure of penile incision after cyst excision
REFERENCES
1. Suwa M, Takeda M, et al. Epidermoid cyst of the penis: a case report and review of the literature. Int J Urol 2000;7:431–433. DOI: 10.1046/j.1442-2042.2000.00219.x.
2. Khana S. Epidermoid cyst of the glans penis. Eur Urol 1991;19:176–177. DOI: 10.1159/000473609.
3. Rattan J, Rattan S, et al. Epidermoid cyst of the penis with extension into the pelvis. J Urol 1997;158:593–594. DOI: 10.1016/S0022-5347(01)64562-2.
4. Little JSJr, Keating MA, et al. Median raphe cyst of the genitalia. J Urol 1992;148:1872–1873. DOI: 10.1016/S0022-5347(17)37054-4.
5. Dini M, Innocenti A, et al. Basal cell carcinoma arising from epidermoid cyst: a case report. Dermatol Surg 2001;27:585–586. DOI: 10.1097/00042728-200106000-00015.
6. Lopez-Rios F, Rodriguez-Peralto JL, et al. Squamous cell carcinoma arising in a cutaneous epidermal cyst: case report and literature review. Am J Dermatopathol 1999;21:174–177. DOI: 10.1097/00000372-199904000-00012.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.